Fat Grafting
Fat grafting was first reported in 1893. For many decades fat was introduced into the recipient areas as a large block of tissue, most of which failed to survive. A significant improvement was initiated in the early 1990’s with the introduction of micrografting. The increased retention of the fat is attributed to insertion of multiple tiny beads which allows more surface area on the fat for oxygenation and metabolite exchange. Fat is commonly harvested from different sites including the abdomen, inner thighs, knee pads or flank area. The incision site is 2-3mm and requires a single stitch for closure. The tissue removed is then placed in a sterile centrifuge, and then the stem cell rich fat is decanted. The fat is then inset through a 1-2mm slit, and laid down in a series of passes. In most cases the incision does not require any stitches, and can be covered by makeup after a few days.
Depending on the location and volume, the procedure is carried out either under local anesthetic, or in larger cases under intravenous sedation. The major issue with all injectable techniques including hyaluronic acid fillers as well as fat, is retention. Three dimensional studies reveals a decrease in the first 6-9 months, followed by a volume rebound towards the second year. These studies reveal that patients younger than 55 have a retention at 2 years of about 53%, and patients older than 55 have about a 31% retention. Therefore, some patients request touch up procedures.
 |
 |
 |
 |
This patient had grafting in the lower lid, cheek, nasolabial fold, and the marionette lines beneath the corner of the mouth. This is a better than average result as not all patients can attain as good a result as this.
 |
 |
 |
 |
Aside from a facelift, much of the improvement has been from structural fat grafting beneath the eyes, cheeks, nasolabial folds, and jaw line.
 |
 |
 |
 |
The post op photos were taken 1 week after the procedure. Even at this time there is minimal bruising, and the entry slits are well covered.
 |
 |
 |
 |
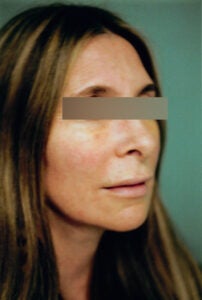
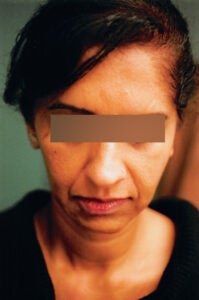
This middle aged woman sustained significant fat loss. She has had grafting to the temples, lower lids, cheeks and nasolabial folds.
 |
 |
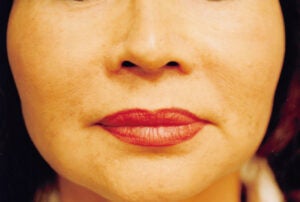
This attractive middle age woman has had grafting around the eyes, cheeks, nasolabial folds and lips.
 |
 |
 |
 |
This patient has had grafting to the lower lids, cheeks, nasolabial folds and chin.
 |
 |
This young woman complained of hollowing beneath the eyes. Two tiny entrance points for grafting were used … one in the upper cheek, and one by the tear trough.
 |
 |
 |
 |
This woman had grafting to her face. The under exposed preoperative photos are used to plan the volume of fat required for each target area.
 |
 |
 |
 |
This young woman complained of “tired lower lids”. Facial grafting was carried out and the lower lids softly brought out with judicious volumes of fat.
 |
 |
 |
 |
Sidelighting has been used in the preoperative photo in order to assess contour problems and then develop a plan as to how much fat gets deposited in the irregularities.
 |
 |
This patient didn’t like the protuberant lower eye bags. Normally this would have been dealt with by sculpting the fat from inside the eyelid. The patient didn’t wish to have this procedure, so we both agreed to graft fat above and below the fullness.
 |
 |
 |
 |
This patient had facial rejuvenative surgery which was augmented by grafting to the lower lids, glabellar area, cheeks and nasolabial folds.
 |
 |
 |
 |
Grafting has been carried out in the intraorbital area as well as the cheeks and nasolabial folds.
 |
 |
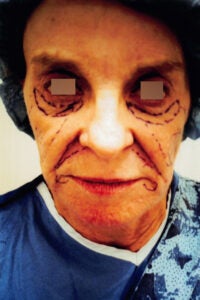
This lovely 69-year-old woman sustained significant loss of volume in her face. The pre-operative insertion patterns are noted. She has had only fat grafting.
 |
 |
 |
 |
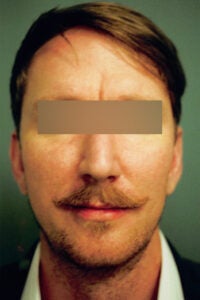
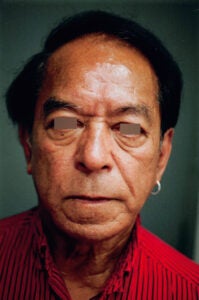
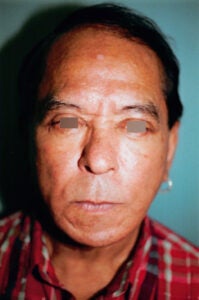
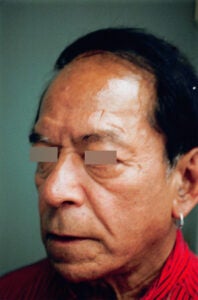
This handsome man has had a facelift and blepharoplasties. In addition his fat compartments have been replenished with structural fat grafting.
 |
 |
 |
 |
This patient has had full face fat grafting. The nasolabial folds have modest results usually attaining a 30-40% improvement, but seldom more.
 |
 |
 |
 |
This elegant woman sustained asymmetric tissue loss, particularly on the right side. Asymmetric injection patterns and volume helped restore her symmetry.
 |
 |
 |
 |
Rejuvenative surgery has been augmented by pan facial fat grafting. Most fat graft patients use a little Tylenol for any discomfort.
 |
 |
 |
 |
This middle aged woman had facial rejuvenative surgery. She had sustained significant deep fat loss and thus was a candidate for asymmetric grafting.
 |
 |
 |
 |
This gentleman had facial rejuvenation surgery enhanced by fat grafting around the eyes, cheeks, and chin.